本帖最后由 老马 于 2013-5-27 03:18 编辑
Clovis Oncology's CEO Discusses Q4 2012 Results - Earnings Call Transcript
Patrick Mahaffy
Thanks, Anna. Welcome, everybody. Thank you for joining us this afternoon. We made very important progress during 2012 despite the disappointing outcome of the LEAP study for CO-101 in pancreatic cancer.
This afternoon, I’d like to take the opportunity to highlight our clinical development programs CO-1686 and rucaparib in the context of 2012 accomplishments and anticipated 2013 milestones.
First to CO-1686, which is our oral small molecule covalent inhibitor of the mutant forms of epidermal growth factor receptor or EGFR for the treatment of non-small cell lung cancer. 1686 targets both the initial activating EGFR mutations, as well as the primary resistance mutation, T790M, and it has the potential to treat non-small cell lung cancer patients with EGFR mutations both as a first-line and a second-line treatment.
The CO-1686 spares wild-type or normal EGFR, it has the potential to cause a lower incidence of toxicity, particularly the skin rash and diarrhea normally associated with other EGFR inhibitors.
In March 2012, we initiated our first human clinical study in 1686. We initiated the Phase I/II study at a dose of 115 mgs per day given once daily and we recently initiated a dosing cohort at a dose of 900 milligrams two times daily.
Based on animal models and PK data, we believe that the cohorts that commenced dosing in late 2012 are now approaching the therapeutic window for 1686 to begin to show clinical benefit. In particular, we’re seeing trough plasma levels above the therapeutic threshold for a reasonable period of time, especially when the drug is given twice daily.
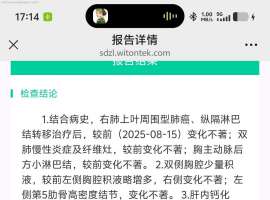
While we have not yet achieved the partial responses defined by RECIST criteria, which requires a 30% shrinkage or greater tumor reduction, we are seeing tumor shrinkage for CO-1686 and T790M positive patients as we get to higher dosing.
As the study has evolved, we’re seeing progressively better patient outcomes as one would expect with dose escalation. Initially, patients stated that they felt better. And as doses got higher we did then begin to see signs of symptomatic relief such as reduced coughs and fatigue. We are now seeing signs of clinical benefit, including reductions in pleural effusions and objective evidence of tumor reduction. Hopefully, this progress will continue as we continue to dose escalate.
We are seeing some reservable grade 1 and 2 toxicities. So we’ve not yet seen rash or diarrhea in the cohorts completed to date as is common with TKI treatment. In fact, at this point, there is no single toxicity that we are seeing that begins to emerge as a dose limiting toxicity, and therefore, we cannot yet predict what a dose limiting toxicity may be. We look forward to sharing preliminary Phase I data from this study at ASCO in early June.
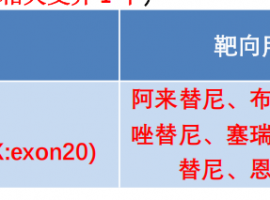
Once we’ve established the optimal dose for 1686, we intend to initiate an expansion cohort of approximately 40 non-small cell lung cancer patients, who have progressed well on treatment with EGFR-directed therapy such as Tarceva or Iressa and have developed the T790M resistance mutation.
We also intend to study 1686 in an expansion cohort of newly diagnosed patients, who express the activating mutations of EGFR. But by inhibiting both the activating mutations of EGFR as well as its primary resistance mechanism, we’re able to demonstrate a meaningful progression-free survival benefit compared to what has been seen to date for Tarceva and other TKI therapies. We will be in a position to move 1686 into a frontline development program.
Pending data from the second line T790M positive cohort, our goal is to commence a registration study in the first half of 2014 in this T790M positive, TKI failure population.
As we previously discussed, we’re developing an improved formulation of 1686. Today, we are using a free base capsule, which is simply active ingredient in a capsule form. The commercial formulation, which we expect to use in the registration study, is the hydrobromide salt tablet. In animal models, this formulation had demonstrated exposure levels between three times and ten times higher than the current free base formulation. So we anticipate that the ultimate human dose will also be lower than that which we’re currently exploring with the free base formulation. We intend to transition this formulation in the patients during the third quarter of this year. Once this new formulation is available and we have determined an appropriate dose, we also plan to initiate a Phase I study in Japan.
Finally, as to 1686, in late January, we entered into an exclusive sub-license to certain patent applications owned by Dana-Farber Cancer Institute (inaudible) inhibitors of the EGFR JT permutation or T790M – already strong position of our CO-1686 patent estate. These patent applications are also known as the gate keeper patent applications.
===============================================================
1期临床中使用的是CO-1686游离碱胶囊,以后打算使用CO-1686氢溴酸盐片。之前的动物模型结果显示,CO-1686氢溴酸盐的血药浓度是游离碱的3-10倍,因此我们预计病人最终使用的剂量将小于临床剂量。我们将在今年第三季度使用新剂型,并在日本开展1期临床试验。CO-1686的专利也属于gate keeper公司。
|
 不知不觉进入第七年。。胸腔积液怎么
中间这几年很顺利也很稳定 这几年都没再关注这个平台。空窗一年半,最近一次复查胸腔
不知不觉进入第七年。。胸腔积液怎么
中间这几年很顺利也很稳定 这几年都没再关注这个平台。空窗一年半,最近一次复查胸腔
 扫清治疗迷雾!赵军教授、刘晓梅教授
作者:雨过天晴“一代药物耐药后,能直接换成新一代药物吗?”“复查发现脑部有几个很
扫清治疗迷雾!赵军教授、刘晓梅教授
作者:雨过天晴“一代药物耐药后,能直接换成新一代药物吗?”“复查发现脑部有几个很
 发生率高达97%!抗癌路上,别让口腔
作者:雨过天晴
口腔黏膜炎作为癌症患者在抗肿瘤治疗过程中最常见的并发症之一,其高
发生率高达97%!抗癌路上,别让口腔
作者:雨过天晴
口腔黏膜炎作为癌症患者在抗肿瘤治疗过程中最常见的并发症之一,其高
 爸爸晚期肺癌肿瘤已经看不到了!我确
讲述者:陈先生整理者:pear
适逢暑假得闲,我带着全家自驾出游,正将最后一件行李塞
爸爸晚期肺癌肿瘤已经看不到了!我确
讲述者:陈先生整理者:pear
适逢暑假得闲,我带着全家自驾出游,正将最后一件行李塞
 肺腺癌10年,伏美替尼 心血管副作用
奶奶78岁,肺腺癌10年,2017.7-2023.7第一代靶向药凯美纳6年,2023.7至今伏美替尼1年
肺腺癌10年,伏美替尼 心血管副作用
奶奶78岁,肺腺癌10年,2017.7-2023.7第一代靶向药凯美纳6年,2023.7至今伏美替尼1年





 显身卡
显身卡


